| |
I will never forget that day my partner and I emerged from
thick jungle vegetation that enshrouded an obscured footpath
with but the faintest idea of what lay ahead. Beneath an enormous
niim tree, a young boy lay listlessly draped over the lap of
his father. With both urgency and extreme care a traditional
healer cleaned and dressed the boy's ulcerated leg with dried
leaves. Alerted to our presence, the father looked up, and
seeing us, his eyes began to swell with tears of hope. The
ulcer was already in the later stages, extending from his inner
thigh to mid-calf. Severe anemia and dehydration further compounded
the gravity of the situation and death seemed imminent. However,
refusing to accept this harsh reality, we transported the boy
to a hospital, hoping we could preserve his life just long
enough for HART surgeons to arrive and perform the complicated
skin grafting procedures that were needed.
Fate, however, seemed
to have her own plans. On a warm Saturday evening, young
Joseph quietly passed away. Words cannot describe how helpless
we
felt as we later explained the young boy's death to his parents.
Unfortunately, with no available vaccine or drug to treat
this horrible disease, this scene will be repeated in countless
villages throughout West Africa. However, each year dozens
of HART volunteers travel to these villages, devoting countless
hours to organizing grass-root community awareness and education
campaigns, conducting social research, training local health
care providers, and performing life saving surgeries. Although
we are far from seeing the end of this disease, we are making
amazing progress. I take great pride in knowing that as a
student
volunteer, I can contribute to this progress. —Parker Fillmore
Student Volunteer
As a plastic surgeon I have been on several mission trips
outside of the United States to operate on various congenital
diseases and acquired deformities. The most valuable trips
for me have been those which included education of the local
medical personnel and people so that the medical/surgical care
I start can be continued. It is one thing to change a single
childs life, but in doing so you educate others to continue
to effect those changes then you have left a legacy.
My operative skills may have helped a few on my trip with
HART to Ghana, but the education of local physicians, the
outreach
to local villages, and the providing of medical equipment
to local hospitals continues to improve care for those
with the
Buruli Ulcer long after I am forgotten. I hope to travel
with HART again soon, and offer my continued support at
any time. —Melinda
Haws, MD

The most important and lasting inpression from our medical
relief trip to Ghana waas the extreme poverty that this West
African nation is faced with. The differences between the medical
care available in the U.S. and Dunkwa, the village in which
we worked, were profound.
For example many patients were lucky if they had a bed rather
than a mat on the floor.
The patients ate only if family or friends could prepare food.
Any medication was a luxury, particularly pain medication.
No lab tests were available.
The operating room had two fifty-year old operating tables
with rusting parts.
The hospital did not have disposable operating room items.
(My guess is that the disposable items we brought were cleaned
and reused upon our departure).
When I feel the stress of a long day's work, I take out my
photo album from Ghana , relive the experiences, say a prayer
of gratitude for my life and hope that our work in Ghana
can continue and grow in magnitude. —Mary Mastin, M.D.
General Surgeon, V.A. Hospital
Salt Lake City, Utah
We would like to comment the benevolent work done by HART
in the control of Buruli Ulcer in the Central Region of Ghana.
This organization has been able to organize both materials
and human resources to offer free medical and surgical care.
We are appealing to others to express the same degree of concern
to contribute personally or channel their support through the
HART team to sustain theri efforts to control the disease in
this area.
—Dr. Erasmus Yao Klutse
District Director of Health Services
Dunkwa, Ghana
Summer In Ghana
The weather was hot, and sweat was dripping down my back, but
I was happy to be there. This was a hospital unlike any other
I had seen, small and in need of repair. I looked out the window
and saw patients dressed in bright African fabric; they waved
hello and beamed welcoming smiles. I had always dreamed of
traveling to Africa as part of a medical team, and I was amazed
I was finally there.
When I was a sophomore in college, I discovered a group called
the Humanitarian Aid Relief Team (HART) that gives students
the opportunity to help patients afflicted with the Buruli
ulcer (a devastating mycobacterium skin-disease) in Ghana.
I started volunteering for the group in October 1999 and
signed up for the next medical trip.
Our team consisted of eight students, three nurses, a nurse
anesthetist, and two general surgeons. Our mission was
to go to the Dunkwa Governmental Hospital and work with
Ghanaian
nurses and doctors to perform debridements and skin grafts
on patients inflicted with the Buruli ulcer. Our first
night, the two surgeons explained that because of the delicate
nature
of the surgeries, although we would help most people with
the
surgeries, we might also be inadvertently hurting a number
of people. That was a risk I had never even considered.
However, it soon became evident that sometimes complications
did arise.
The important thing, though, was that the good we could
accomplish outweighed the bad.
It was fascinating participating in the surgeries. As students,
we alternated between prepping the patients for surgery,
assisting the doctors in the operating room, and nursing
the patients
in the recovery room following surgery. Each morning
many more people lined up to receive surgery than we could
possibly
operate
on during our stay. On my way to the isolation ward,
patients would plead with me to help them. I felt envious
of the
doctors and sad that I didn’t have the knowledge or capability
to help. I realized I would never feel like I was living life
fully if I weren’t helping people in a medical profession.
One small girl named Caya touched me deeply. She had
a very serious case of Buruli on her leg that prevented
her
from
walking, and she was weak and sickly. The operations
were traumatic
for Caya. White-skinned Americans, wearing masks and
speaking a foreign language, would take her to a room
full of strange
equipment and cause her additional pain. It got to
the point that whenever members of our team entered the
isolation
ward,
she would cry. We successfully performed three or four
surgeries, but the day before we left she contracted
a bacterial infection
that caused her skin grafts to go bad. Nevertheless,
the morning we left she handed me a small metal bowl,
covered
with a white
doily and containing a dozen or so small eggs, neatly
lined up. I realized what a privilege it is to offer
medical
services to people
This past summer I returned to Ghana to study the people’s
beliefs regarding the origin of the Buruli ulcer, what kind
of treatments they seek, and what hardships Buruli causes in
their daily lives. It was amazing to live in the people’s
element, away from electricity, running water, transportation,
and even medical treatment. Many people assumed we were medical
doctors and came to us with their problems—Buruli, fevers,
body aches, tumors, etc.—only to be told we were students
who didn’t have the knowledge and ability to treat them.
It was hard to be tied down in these situations because of
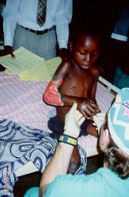
ignorance. One especially humbling case was a three-year-old boy who
had been having convulsions. His parents took him to one
of the
fetish priests to see if he could treat the convulsions,
and the priest agreed to let us observe some of the healing
ritual.
When we came on the scene, a small group of people were gathered
around a small cauldron and were splashing water all over
the small boy’s body. He was only semi-conscious, and his
body was limp and pale. I immediately recognized that the situation
was critical and the boy was teetering toward death. I felt
helpless, so I encouraged the people to hire a taxi to take
the boy to the hospital two hours away—but I feared the
boy wouldn’t make it. More than ever, I wished I were
a doctor. I very much wanted to help this boy. The next morning,
our translator informed us that the boy died only minutes after
he arrived at the hospital. If I were a trained physician,
would I have been able to save this child’s life? It is a privilege to live in a place where education is readily
available and opportunities abound. I want to take advantage
of this knowledge and go to medical school to become a physician,
and with this knowledge I want to make a difference in individual
lives, both at home and abroad. It takes training, it takes
ability, and it takes desire. Helping others who are suffering
physically and emotionally is a sacred privilege, and I will
dedicate my life to it. —Jeff Bigelow
President of HART Volunteer Chapter
|